Nearly half of all deaths and about a third of disabilities in low and middle-income countries could be avoided if people had access to emergency care. In Africa the main causes of emergencies are road accidents, obstetric complications, severe illnesses and non-communicable diseases.
Over the past 18 years the African Federation for Emergency Medicine, an advocacy group, has been encouraging the development of emergency care systems on the continent. The gaps it has identified include decent transport and hospital services.
But to address these challenges data is needed on the number of hospitals, their locations as well as the population marginalised. Most countries in Africa don’t have this information. They lack basic inventories of health care service providers, including the number of hospitals.
Our study set out to address this problem by producing the first ever assessment of hospital services in sub-Saharan Africa, and used it to work out peoples’ access to care.
Get your news from people who know what they’re talking about.
Get newsletter
The results – including how long it takes to get to a hospital – show where investment is needed in improving access. Various interventions are necessary. These should include building new hospitals, improving ambulatory care, building new roads and fixing existing ones.
But the most urgent action is that countries must update their hospital lists, including assessment of capacity and capability to provide emergency care and updating of the private sector. Our research goes someway to helping them start this process. We have built a database which can be accessed for free and used for assessing service availability at national levels.
Building the database
The hospital list covers 48 countries and islands of sub-Saharan Africa.
To develop the list we used numerous sources for the data, including ministries of health, health information systems, national and international organisations from all the countries and islands. In most cases, the sources were available online but we also relied on personal contacts to obtain hospital data in some countries.
Close to 50% of the hospitals on the list didn’t have GPS coordinates that could aid in precisely locating them. To overcome the problem we assigned them unique location attributes using online mapping tools such as Google earth and OpenStreetMaps.
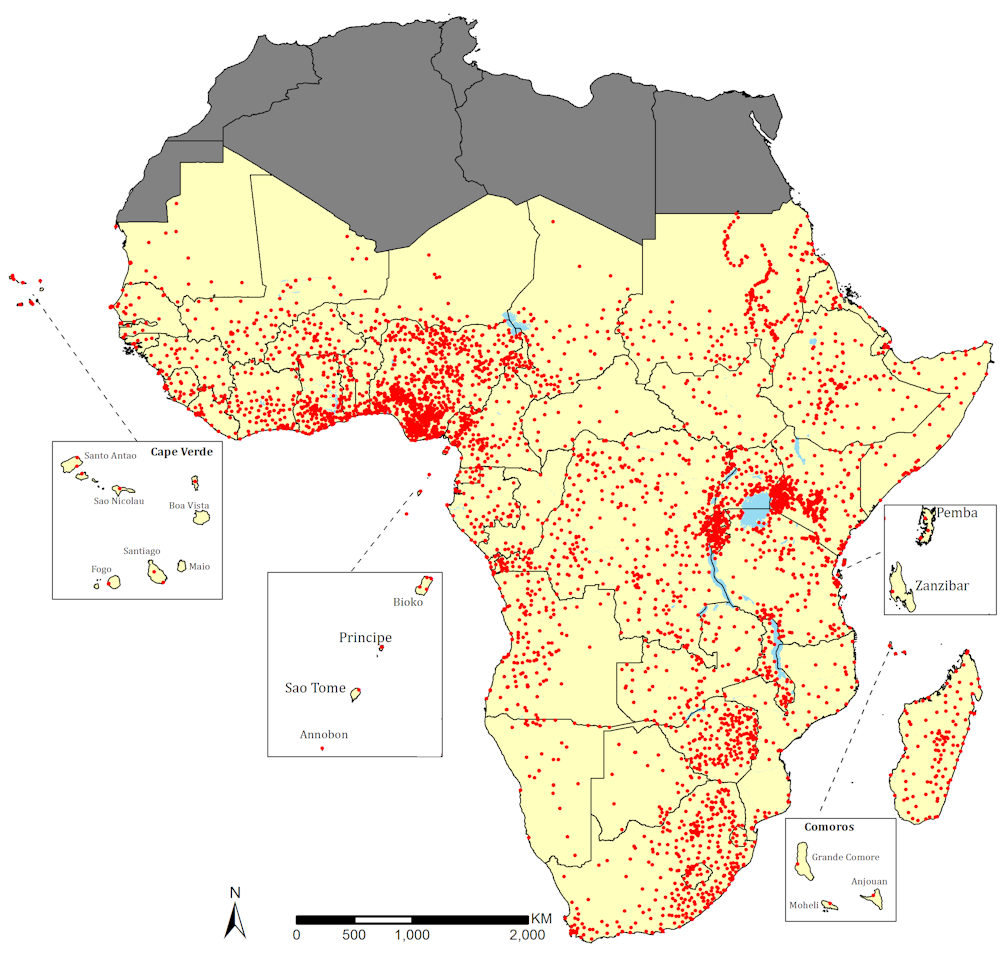
This audit located 4908 public sector hospitals which were precisely assigned location attributes (Figure 1).
Nigeria, which accounts for close to a fifth of sub-Saharan Africa’s population had the highest number of hospitals at 879. Other countries with significantly high numbers of public hospitals were the Democratic Republic of Congo (435), Kenya (399) and South Africa (337).
The least were in smaller countries such as Cape Verde, Zanzibar, and São Tomé and Príncipe. This information was used as a starting point to calculate the geographic access to the hospital services.
Timely access
We measured geographic accessibility by travel time to the nearest public hospital. We did this by calculating how long it would take to travel by road based on the major means of transport in the region.
We assembled road networks from Google earth and OpenStreetMaps, and assigned travel speeds along the roads. We then developed a model that calculates the time it would take for a patient to travel from any 100m by 100m square grid of location to the nearest hospital.
More specifically, a significant proportion of women need access to hospital care when in labour and we additionally determined how long they would take to get to the nearest hospital.
Results reveal that, less than a third (29%) of the total population and 28% of the women of child bearing age, lived more than two hours from the nearest hospitals. The two-hour threshold is a widely used recommendation by the WHO and the Lancet Commission for global surgery for defining access to emergency obstetric and surgical care respectively. In addition, international benchmarks by the Lancet commission for global surgery recommends having 80% of any given population within two hours as critical in ensuring universal health coverage by 2030.
The most surprising outcome was the huge differences between countries. For example, more than 75% of the population in South Sudan lived outside the two-hour threshold. Other poorly served countries included Central African Republic, Chad and Eritrea. More than half of their populations lived outside the two-hour threshold.
The best served countries were mostly islands like Zanzibar, Comoros and São Tomé and Príncipe. More than 95% of their populations were within two hours of a hospital. Large countries such as Kenya, South Africa and Nigeria also had good access indices, with more than 90% within the two-hour band.
All 48 countries in our survey have signed up to the sustainable development goal of delivering universal health care by 2030, part of which involves access to hospitals. Our research can help countries work out what they need to do to make this a reality when it comes to emergency care. There’s still a long way to go. Only 16 countries in our survey achieved 80% coverage in access to a hospital within two hours.